

This edition of Capitol Beat is co-authored by Billie Lynn Allard, a nurse innovator and leader in Vermont. Ms. Allard founded and now directs a transitional care program that is a core component of the Accountable Community of Health of the Southwestern Vermont Health Care system.
Honors to rural nurses! November 21 is National Rural Health Day, a reminder of the unique challenges that people are facing — and nurses are meeting — in less populated parts of the country.
Improving health and access to care in rural areas for the 60 million Americans who live there should be a priority in a rapidly changing health care system. Due to several facts of rural life, we see significant differences between rural and non-rural residents when it comes to health. For people in rural areas, health disparities can mean greater burdens of severe disease like cancer and heart disease. There are also higher rates of injury and suicide in rural areas versus non-rural areas.
Often, accessing care is a serious challenge for people in rural areas, where traveling to appointments can be difficult, and lack of health care coverage can also be a barrier. Some rural residents may avoid care where they live because they fear stigma and loss of privacy, for instance, if they are living with opioid use disorders, HIV, or mental health conditions. When there are not enough health care providers to meet the needs of rural communities, access is more restricted still.
There is good news for rural health, however.
The good news is that nurses can frequently be found leading their communities to drive transformative solutions. An example is the team-based care model forged by nurses in southwestern Vermont. Billie Lynn Allard, MS, RN, FAAN, and director of the program, shares her story:
I am fortunate enough to work in an ANCC Magnet-recognized community hospital where visionary leadership has supported our efforts in transforming care delivery to better meet the needs of the 75,000 people who live in our service area. That area, covering parts of Vermont, New York and Massachusetts, is largely rural. Our initiative has redeployed hospital-based nurses to expand primary care capacity and focus with community partners on high-risk, high-cost patients who have complex care needs.
From the beginning of this effort, transitional care nurses navigated our rural care system along with patients, in order to experience care delivery through their eyes. Our goal was to identify gaps in care coordination, communication, education and access to resources that were negatively affecting health in our community. Then, we proactively met with home care agencies, skilled nursing facilities, and community agencies to share information and find collaborative ways to improve care coordination across our community, avoiding overlap, duplication, waste or competition.
For the first time in our nursing careers, we were able to understand why so many patients were not successful at managing their chronic disease, causing multiple preventable emergency visits and hospitalizations. We acknowledged that silos of care delivery hamper any patient’s ability to understand how to take their medications correctly, and what to do when their symptoms worsen. We were overwhelmed by the role of social determinants of health (SDOH) causing so many patients to have to choose between food, heat, or medication. We witnessed clearly what Maslow’s Hierarchy of Needs taught us in nursing school — that people need adequate food, water, and shelter to achieve optimal health. We saw where we were falling short in our care coordination, as patients went home from the hospital without meaningful resources to manage their health.
In the past six years, we have systematically and effectively built relationships across our community. Transitional care nurses now regularly make home visits to high-needs patients, which has resulted in a 50 percent reduction in hospitalizations. Interdisciplinary teams are creating integrated care plans for individuals who had previously accessed the hospital seeking to meet their needs for food, shelter and social support. New pilot programs are testing out the use of clinical pharmacists in primary care practices, and physical therapists are available in the emergency department. The opening of the PUCK (Pediatric Urgent Care for Kids) center has led to improved management of high-risk children requiring mental health assessment and support. An opioid task force is increasing services available and advocating for funding. Screening of high-risk children and adults with immediate access to support is uncovering huge opportunities.
Our providers are becoming proficient in longitudinal care delivery, considering what happened before and after each patient touch in order to reach the best possible results. Step by step we are making progress and without a doubt, it is truly the most rewarding part of our careers! We must meet people where they are, embracing the role of SDOH. We must empower them to make informed decisions based on what matters to them.
Nurses are leading transformation of rural care delivery, and every day we are witnessing the difference it makes, as we seek to meet the Quadruple Aim of health care: Improve patient experience, improve the health of our community, lower costs, and improve the experience of the care giver.
ANA advocates at the federal level to augment and promote nurse-led innovation in underserved rural areas. For instance, in a recent letter to the Health Resources and Services Administration (HRSA), ANA urged more federal support for innovative models like the Accountable Community of Health in Vermont. The letter also suggested HRSA should consider ways of incentivizing states to reform nurse practice laws so that all nurses can practice to the full extent of their education and clinical training.
To support nurse advocacy in rural health, the following resources may be helpful:
- Social Determinants of Health: What Every Nurse Should Know
- Cross-Continuum Collaboration in Health Care: Unleashing the Potential
- American Academy of Nursing’s Edge Runner programs
- State resource guides
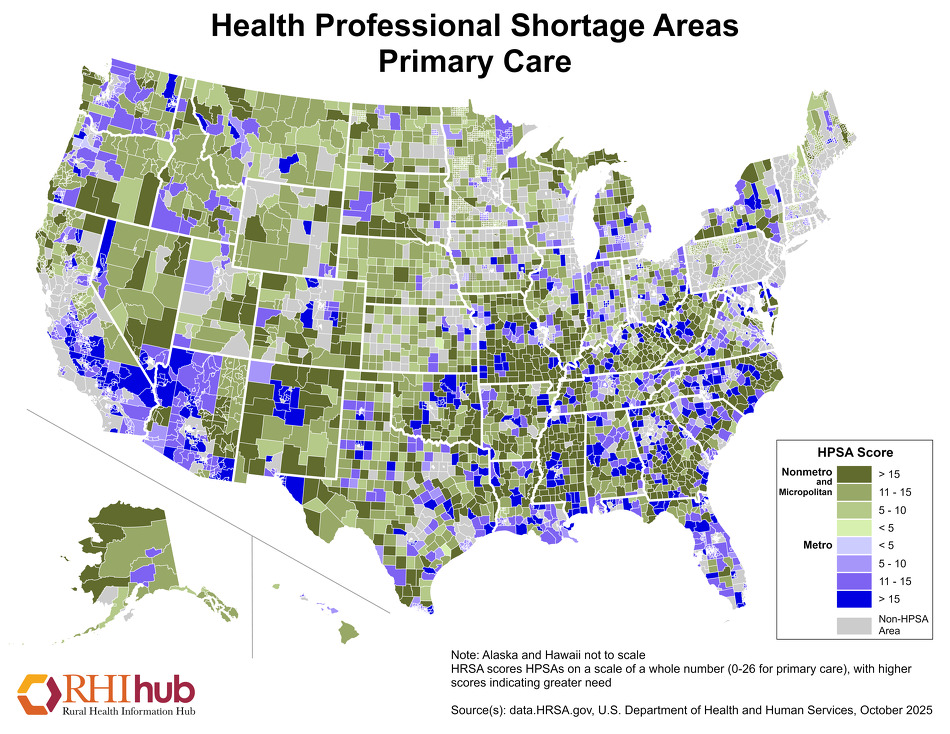
- Map of primary care shortage areas
- Rural Suicide Prevention Toolkit
- Power of Rural Campaign
- Telehealth resources
{kind=link}
Let us know if you have a story of #RNAction in rural health. Send a message to gova@ana.org.