

Ad Nauseum is a Latin term describing something that has continued “to the point of nausea.” Merriam-Webster defines it as “to a sickening or excessive degree.” Ad Nauseum, then, holds the distinction of being the perfect word to describe the current status of research demonstrating the safety and efficacy of Advanced Practice Registered Nurses (APRNs).
As one nurse put it, “we may be the most studied profession out there. You certainly don’t see dentists being required to justify their practice through hundreds upon hundreds of studies over the course of decades before they are allowed to practice to fullest extent of their license.”
It’s been six years since the National Academy of Medicine concluded in its groundbreaking “Future of Nursing” report that “the contention that APRNs are less able than physicians to deliver care that is safe, effective, and efficient is not supported by the decades of research that has examined this question.” The Institute backed this up with mountains of peer-reviewed scientific evidence.
Since then, the evidence has continued to pour in. Kleiner, Park, and Wing found in 2014 that “more restrictive state licensing practices [for APRNs] increase the costs of medical care… and do not appear to influence health care quality….” Xue, Ye, Brewer, and Spetz found in a systematic literature review that “removing restrictions on NP scope of practice regulations could be a viable and effective strategy to increase primary care capacity.” Kurtzman et al concluded in 2017 that “[Nurse practitioner, ‘NP’] care is comparable to physician care in most ways and…the quality of NP-delivered care does not significantly vary by states’ NP independence status.”
These studies are just a smattering of scores of research published since the National Academy of Medicine, on the basis of decades of research, concluded without stipulation that APRNs practice just as safely, effectively, and efficiently as physicians.
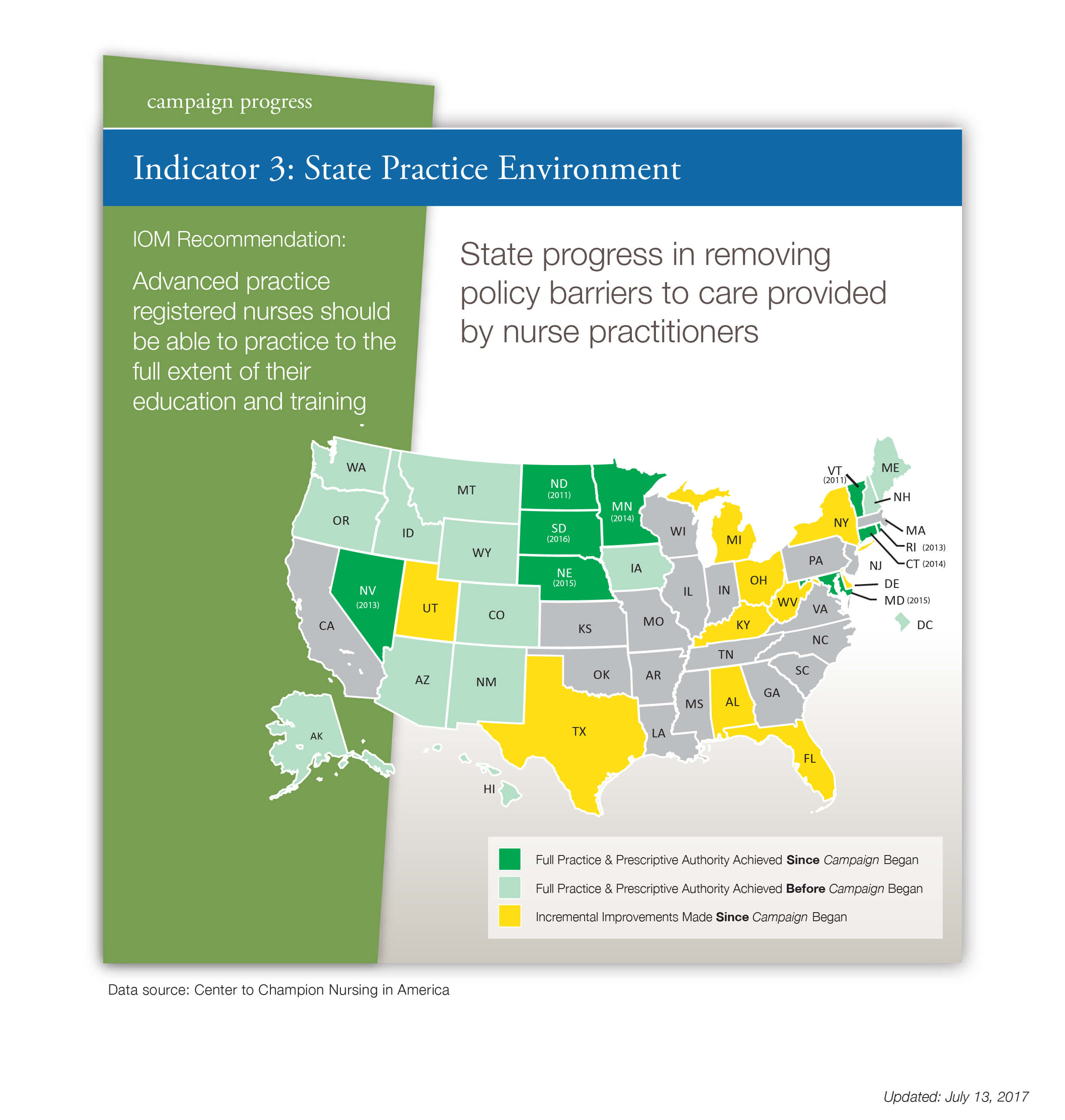
And yet, 28 states still do not allow APRNs to practice to the full scope of their training and education. The VA recently allowed APRNs full practice authority, but excluded nurse anesthetists.
{kind=link}
This is not for lack of effort. Nurses, consumers, patients, and advocacy groups have collaborated in various ways to ask legislators in the 28 states to allow full APRN practice in the interest of achieving the “triple aim” of improving patient outcomes, population health, and per capita cost. The Robert Wood Johnson Foundation, AARP, the FTC, the National Governors Association, and many other influential voices have also weighed in on the side of granting full practice authority to APRNs in all US states.
In many cases, these efforts have been thwarted by legislators and others who demand more evidence. But when decades of research ad nauseum clearly demonstrate the safety and efficacy of full APRN practice, many patients and nurses find themselves wondering: when is enough, enough?
Obviously, states influenced by moneyed lobbyists will reflect restrictive structures that will continue to affect the health of this nation, whether it is restricting CNPs or continued pollution of our air and water sources. Each nurse needs to wake up to the realization that not all our representatives at the local, state or national levels represent nurses unless there are the donor dollars to back it up.
I have experienced and seen firsthand the problems that arise from NP’s not being able to practice to their full scope. In my state we have to have a collaborating physician agreement. In our office it is the MD and me. When he is gone, some orders that NP’s are not allowed to sign yet, such as PT/OT orders for after discharge, this can delay the patient’s discharge until the MD is back and signs them. Sometimes I have seen the patient and he hasn’t, so he is signing orders on someone he hasn’t even seen, but that is ok apparently with the powers above. This wrong and puts the MD in a not so comfy spot and it’s not fair to all parties involved. NP’s should be able to practice to their full scope. We know when to consult an MD on issues that arise, just like MD’s consult other MD’s/specialists when they need feedback and advice. The MD I work with even acknowledges that NP’s have some training that MD’s don’t, such as more in depth psyche interaction because of our previous nurses training. In my state’s RN programs, we have to be able to conduct a group session and 1:1 therapeutic interactions to pass our psyche clinicals. The MD I work with said that in medical school, they do not go that in depth into the psyche rotation. They focus on diagnosing and treating unless they choose that as their specialty. As a former cardiology nurse, I also had more experience reading EKG’s than he did as well. Let us practice to our full scope and be a true full member of the health care team!
Perhaps the reason malpractice rates for APNs remain low is that it is generally the supervising our collaborative physician who beats the liability for the errors committed since they are the “deep pockets.” When APNs achieve the independence they are fighting for they will also assume the complete liability and malpractice rates will rise accordingly.
See Lisa Summers 2007 editorial “Enough is Enough!” about certified nurse-midwives Time to update this for all APRN roles…
http://onlinelibrary.wiley.com/doi/10.1016/j.jmwh.2007.06.019/abstract